
Dooley Noted: 4/20/2015
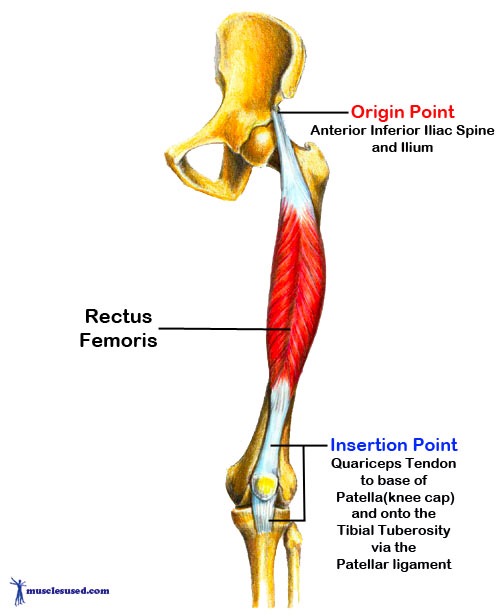
Rectus Femoris (RF) is a glorious, long muscle that crosses both the hip joint and the knee joint.
RF has similarities with the rest of quadriceps femoris. It shares an innervation in the femoral nerve (L2-L4) and a common distal attachment onto the tibial tuberosity. As a quad does well, RF extends the tibia.

With the major spinal level being L4, the innervation is more seldom compromised by disc herniation. This is opposite the antagonist glutes and hamstrings. These receive their major spinal levels from the most herniated levels of the lumbar spine, affecting L5, S1 nerve roots.
Thus, quadriceps dominance is a dysfunctional crutch of working in an imbalanced fashion in disc herniation patients.
RF does not tend toward facilitation, like most two-joint muscles. It has no attachment to the femur. Unlike the vastus muscles of quadriceps femoris, RF exerts its tibial pull relative to the ilium of the pelvis.
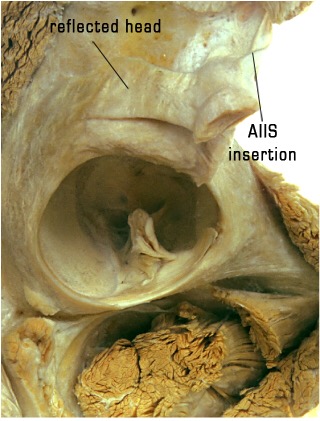
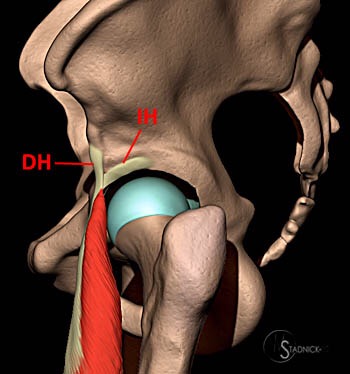
RF has two proximal attachments. The most commonly recognized is the attachment onto the anterior inferior iliac spine, just inferior to the attachment of sartorius.
The often forgotten reflected head of RF attaches to the acetabular rim, anchoring itself to the anterolateral joint capsule as it inserts deep to gluteus minimus.
These anterior hip attachments help to flex the lower extremity relative to the pelvis.
This movement is usually referred to as hip flexion, but it’s not quite the same pull as powerful hip flexors like the adductors and iliacus.
This is because RF doesn’t attach to the femur. It’s in a potentially weaker class of hip flexors, like sartorius, tensor fascia lata, psoas, and gracilis. These muscles all cross more than one joint, so they are slaves to what is also happening at the opposite attachment.
The reflected head of RF is much like the long head of biceps brachii, and I liken them to be analogous at different limbs. RF’s attachment to the acetabular rim near the labrum mimics long head bicep’s glenohumeral labral attachment.
Thus, labral tears can often be perpetuated by stretch-weakening of these muscles.
A common population to get femoroacetabular labral tears is the sprinting population. If the pelvis is stuck in an anterior pelvic tilt, the reflected head of RF becomes stretch-weakened, as the runner repetitively attempts hip extension.
I cringe when I see people in an anterior pelvic tilt (i.e., most people) stretching their quads in the traditional way.
They grab their foot and peel it behind them, getting a stretch of the vastus muscles. But if they have an anterior pelvic tilt, they yank on their reflected head near the labrum, increasing their chances of hip instability and labral tears. (see below)

It’s a quick fix. Make sure the pelvis is neutral with an extended femur.
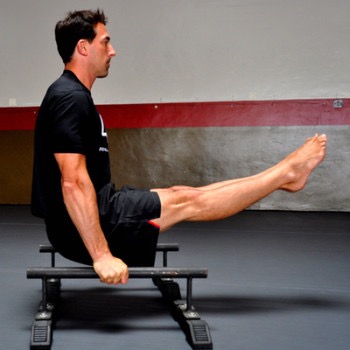
One of the best ways to strengthen RF is to keep the knee extended but flex the lower limb relative to a neutral pelvis. This is exhibited in a standard hanging leg raise. (see below)
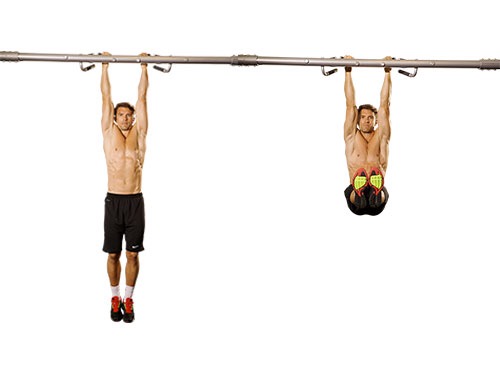
If this is too simple, you can progress to the L-Sit from the floor, from rings or from paralettes.
In whatever exercises or stretches you choose, please consider your goals.
And always consider the anatomy.
Set yourself up for success, instead of setting yourself up for stretch-weakening or muscle tears.
As always, it’s your call.
– Dr. Kathy Dooley